Speech Sound Disorder
SSD is not a diagnosis, but a category heading or umbrella term
Articulation versus Phonology
Phonology is not a technical term for speech
Dr Sean Pert
Historical context
Prior to the 1980s, almost all speech sound disorder work was articulation-based. That is, based on the "Traditional Approach" (Van Riper, 1954). This included the familiar establishment of a single consonant (C) and then building up the word using CV. VC and CVC combinations. This was often slow going work. In addition, children did not always generalise 'contracted words' into their everyday realisation of words, suggesting that some other mechanism was at play.
The advent of Phonology, where it was recognised that children made speech errors at word level, despite being able to produce the target sound in isolation, showed that the majority of speech errors were psycholinguistic in nature, and not attributable to motor speech difficulties.
Unfortunately, many practitioners and services confuse the term 'Phonology' to mean the scientific name for speech. It is a nonsense to have a 'Phonology Care Pathway' for children with speech sound disorder. Children are likely to have Articulation Disorder AND a Phonological Disorder.
Articulation therapy (placement, ear training) fell out of fashion. At the same time, failing to check the child's single sound realisation (stimulability), meant that phonological therapy methods are often misapplied to Articulation Disorder.
In reality, children need therapy for the level(s) of breakdown in the speech chain:
Prior to the 1980s, almost all speech sound disorder work was articulation-based. That is, based on the "Traditional Approach" (Van Riper, 1954). This included the familiar establishment of a single consonant (C) and then building up the word using CV. VC and CVC combinations. This was often slow going work. In addition, children did not always generalise 'contracted words' into their everyday realisation of words, suggesting that some other mechanism was at play.
The advent of Phonology, where it was recognised that children made speech errors at word level, despite being able to produce the target sound in isolation, showed that the majority of speech errors were psycholinguistic in nature, and not attributable to motor speech difficulties.
Unfortunately, many practitioners and services confuse the term 'Phonology' to mean the scientific name for speech. It is a nonsense to have a 'Phonology Care Pathway' for children with speech sound disorder. Children are likely to have Articulation Disorder AND a Phonological Disorder.
Articulation therapy (placement, ear training) fell out of fashion. At the same time, failing to check the child's single sound realisation (stimulability), meant that phonological therapy methods are often misapplied to Articulation Disorder.
In reality, children need therapy for the level(s) of breakdown in the speech chain:
- For Articulation Disorder, placement therapy is indicated for single phone realisation if they cannot produce the phone on target.
- Phonological (meaning-based) therapy is required if the child is stimulable for phones but cannot use them in words.
- The Speech and Language Therapist must be careful not to attribute phonological explanations to articulation disorder and vice versa.
Stimulability: Is the child stimulable for [phone]?: A definition of Articulation Disorder
The Speech and Language Therapist can check if a child is stimulable (is able to imitate a sound on request) by saying the single phone to the child and asking them to repeat it, such as "Say [s]"
If the child is successful, we say that The child is stimulable for [s].
Note the square brackets - single phone production is in square brackets as it is around that has actually been realised/heard, and single sounds have no meaning when realised in isolation.
If the child cannot imitate a single phone after an adult model, then we say that The child is NOT stimulable for [s].
The error type
Distortions: If the child realises a phone that is not a phoneme of that language, then it is called a distortion. For example, in English, a child might realise [s] as [ɬ] or [ç]. Neither of the resulting phones are part of English phonology, and so change in meaning occurs. The listener might say the child is "unclear" or, more commonly, "has a lisp", but the child's word production is not affected in terms of being understood. This is because there is no loss of contrast.
Phonological Implications: If the child realises a phone that IS a phoneme of that language, then the error will have phonological implications. This is because the listener is likely to think that the child is saying another word of English. Contrast is reduced, but for Articulatory reasons (not phonological). For example, if a child realises [s] as [t] at sound level, then in words, misunderstanding might occur, such as the word 'sew' realised as "toe" (the vowel is the same in these words).
In the last example, if the Speech and Language Therapist only assesses word production, they would inadvertently misdiagnose the presence of a phonological process called stopping, when in reality, the difficulty is Articulation Disorder with Phonological Implications. This is problematic, as phonological word-level therapy is unlikely to resolve an articulation problem!
The Speech and Language Therapist can check if a child is stimulable (is able to imitate a sound on request) by saying the single phone to the child and asking them to repeat it, such as "Say [s]"
If the child is successful, we say that The child is stimulable for [s].
Note the square brackets - single phone production is in square brackets as it is around that has actually been realised/heard, and single sounds have no meaning when realised in isolation.
If the child cannot imitate a single phone after an adult model, then we say that The child is NOT stimulable for [s].
The error type
Distortions: If the child realises a phone that is not a phoneme of that language, then it is called a distortion. For example, in English, a child might realise [s] as [ɬ] or [ç]. Neither of the resulting phones are part of English phonology, and so change in meaning occurs. The listener might say the child is "unclear" or, more commonly, "has a lisp", but the child's word production is not affected in terms of being understood. This is because there is no loss of contrast.
Phonological Implications: If the child realises a phone that IS a phoneme of that language, then the error will have phonological implications. This is because the listener is likely to think that the child is saying another word of English. Contrast is reduced, but for Articulatory reasons (not phonological). For example, if a child realises [s] as [t] at sound level, then in words, misunderstanding might occur, such as the word 'sew' realised as "toe" (the vowel is the same in these words).
In the last example, if the Speech and Language Therapist only assesses word production, they would inadvertently misdiagnose the presence of a phonological process called stopping, when in reality, the difficulty is Articulation Disorder with Phonological Implications. This is problematic, as phonological word-level therapy is unlikely to resolve an articulation problem!
Essential components of Speech Assessment for accurate diagnosis of Speech Sound Disorder
SPEECH SOUND DISORDER (SSD) is not a diagnosis. It is a category or umbrella term and must be replaced with an accurate specific diagnosis based on the speech behaviours of the child following careful assessment. Without ALL of the following ESSENTIAL steps, misdiagnosis is highly likely. This results in therapy being less effective, or in some case completely ineffective, since the therapy is not addressing the correct level of breakdown in the speech chain.
Speech and Language Therapists and Services who cut down on these assessment steps should urgently reevaluate their procedures.
Speech and Language Therapists and Services who cut down on these assessment steps should urgently reevaluate their procedures.
No one has ever heard or said a phoneme
Dr Sean Pert
- Single word naming
- Repetition of at least 10 words from the original list to detect any word inconsistency
- Stimulability of single phones - errors made at word level
- Either:
- Phonological assessment - 50 word sample
- OR
- Inconsistency assessment
- Speech systems examination - looking at the structures of the vocal tract to identity any physical / structural abnormalities, such as missing dentition, or cleft lip and/or palate
- Connected speech sample
- Optional (depending on clinical observations):
- Oro-motor assessment
- DDK rates
Phonological simplification processes are NOT real. Children don't think "I will change this fricative into a plosive - the child doesn't realise that a fricative is required
Dr Sean Pert
Many screen do not satisfy the above criteria, or do not make them explicit.
The Diagnostic Evaluation of Articulation and Phonology (DEAP) includes all these elements, and is a full speech sound disorder assessment (rather than a screen).
Accurate diagnoses
The following diagnostic labels are based on Dodd's model of speech sound disorder. This model is widely used due to the following factors:
- based on research, where case studies of real children with SSD have been assessed and successfully treated based on the level(s) of breakdown within the speech chain
- the model covers all children with SSD
- the model is robust and predicts behaviours
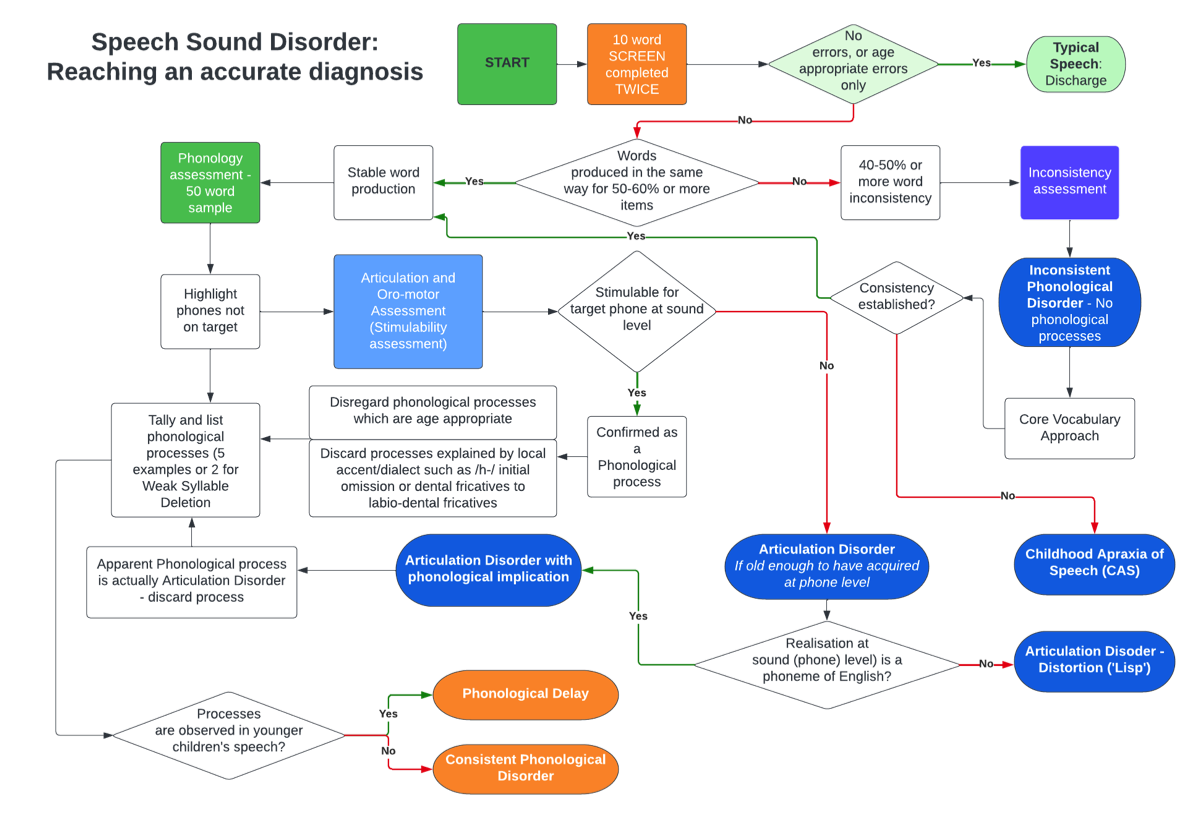
- Articulation Disorder - Not stimulable for one or more phones at sound level, and is old enough to have acquired those phones. Note that children may occasionally use an on-target phone in words or connected speech, but if they are not able to (consciously) repeat a phone on demand, then they do not have sufficient control over their speech and would still be deemed to have Articulation Disorder. Note that there is no such thing as '*Articulation Delay'.
- PHONOLOGICAL DISORDERS: This is a category of the following disorders. Note that there can be ONLY ONE PHONOLOGICAL label
- Phonological delay. The child makes speech sound substitution errors, or structural errors which are observed in younger children's speech.
- Examples include:
- substitution errors such as Voicing, Fronting, Stopping of fricatives, Deaffrication, and
- structural errors such as Final Consonant Deletion, Weak Syllable Deletion, Cluster Reduction.
- The normative data should be based on the child's own speech community.
- In the UK, the largest sample of typically developing children's speech was undertaken by Dodd et al. (2003)
- Note that US and some other communities analyse simplification errors differently and may include normative data based on their own local populations, which may be similar, but not the same as UK data. Processes unfamiliar to UK Speech and Language Therapists may be employed, such as Alveolarization.
- Accent differences such as different vowels, initial /h/ omission, glottal stop allophone usage for syllable/word final for /t/ and the use of labiodental fricatives [f], [v] for dental fricatives [θ], [ð] are some examples which would not be aims for treatment, but rather valued as essential components of a person's accent/dialect and identity.
- Phonological delay is highly unlikely to resolve on its own without professional Speech and Language Therapy intervention.
- The term applies to the child's speech patterns, not to them as an individual. That is, in reports the Speech and Language Therapist should say "Simplification patterns of Phonological Delay are observed in X's speech"
- Consistent Phonological Disorder. The child makes substitution errors, or structural errors NOT found in the speech of younger children.
- May be diagnosed at any age.
- Examples include backing, initial consonant deletion and favoured sound.
- Inconsistent Phonological Disorder (IPD). WORDS are produced differently on each occasion.
- Typically developing children may have up to 40% inconsistency, but above this IPD should be considered.
- Children with IPD do NOT HAVE PHONOLOGICAL PROCESSES and Speech and Language therapists should not attempt to analyse speech simplification in this way of the child has high levels of inconsistent production.
- Inconsistency applies to WORD production, not the use of a phoneme. Children who appear to use phones differently in different word positions may actually have rules based on word position (phonotactic).
- Other motor speech disorders:
- Dysarthria
- Childhood Apraxia of Speech (CAS). This is an extremely rare condition (fewer than one in 1,100 children referred to speech and language therapy) (Broomfield & Dodd, 2004) and is often over-diagnosed, especially if word consistency has not been examined.
- CAS is often confused with Inconsistent Phonological Disorder (IPD)
- CAS was previously known as Developmental Verbal Dyspraxia (DVD) in the UK.
Normative data involves comparing the speech of the child being assessed with that of a representative group of children from the same speech community.
This means it is important to compare a child growing up in the UK with other monolingual English speaking children from the same community.
The button above links to Dodd et al. (2003) normative data used on the Diagnostic Evaluation of Articulation and Phonology (DEAP) assessment.
You may encounter other normative data sets, but these are often not applicable to children growing up in the UK.
Severity does not tell you the diagnosis. It is the TYPE of errors that indicate the breakdown(s) in the speech chain.
Dr Sean Pert
References
Broomfield, J., & Dodd, B. (2004). Children with speech and language disability: caseload characteristics. International Journal of Language & Communication Disorders, 39(3), 303-324. https://doi.org/https://doi.org/10.1080/13682820310001625589
Dodd, B., Holm, A., Hua, Z., & Crosbie, S. (2003). Phonological development: a normative study of British English-speaking children. Clinical Linguistics and Phonology, 17(8), 617-643. https://doi.org/https://doi.org/10.1080/0269920031000111348
Van Riper, C. (1954). Speech Correction: Principles and Methods. Prentice-Hall.
Broomfield, J., & Dodd, B. (2004). Children with speech and language disability: caseload characteristics. International Journal of Language & Communication Disorders, 39(3), 303-324. https://doi.org/https://doi.org/10.1080/13682820310001625589
Dodd, B., Holm, A., Hua, Z., & Crosbie, S. (2003). Phonological development: a normative study of British English-speaking children. Clinical Linguistics and Phonology, 17(8), 617-643. https://doi.org/https://doi.org/10.1080/0269920031000111348
Van Riper, C. (1954). Speech Correction: Principles and Methods. Prentice-Hall.